CMS announced it will continue with its 0.16% rate cut for Medicare Advantage plans insurers.
The Medicare Advantage rate cut proposed in January is here to stay, and payers are not happy.
CMS announced the finalization of the 0.16% rate decrease on Monday, to the disappointment of payers and their investors.
Insurer stocks immediately began to drop, with Humana seeing a nearly 10% drop, CVS Health dropping 5.9%, UnitedHealth decreasing by 4.5%, and Elevance dropping 4%. The stock performance plays into the growing concern amongst investors that Medicare Advantage will continuously face more regulatory and earnings pressure in the future.
With the new rate, next year Medicare Advantage payment cuts could drop by 1% per month per beneficiary, according to a study from the payer lobbying group Better Medicine Alliance, which represents payers in Medicare.
What does it all mean?
Medicare Advantage has seen an unusual rise in medical costs recently, with higher utilization to blame, and insurers are arguing the CMS did not factor in these rising costs that plans are facing when it calculated the new rate. Some payers are arguing that the new rate will hurt seniors, who have been responsible for the higher utilization rates that Medicare Advantage has been seeing.
Medicare Advantage has been a hot topic as of late, with several factors shaking up the market and feelings of uncertainty about how the market will perform in 2024 and 2025. The Biden Administration’s crackdown on upcoding practices is one factor that slowed the original excitement and popularity around Medicare Advantage.
Just last week HealthLeaders reported on the strength of the Medicare Advantage market, with a Chartis study revealing strong potential and stability as enrollment grows. The growth comes on the heels of a big Medicare Advantage milestone: over 50% of Medicare-eligible persons enrolling in a Medicare Advantage plan. With these factors, the optimism of insurance executives prevails.
Other influential factors include an aging population that will most likely continue the high utilization rates. Procedures like knee and hip replacements for seniors are two of the main operation utilizations that are seeing an uptick. Tougher star ratings have also played into the Medicare Advantage payer landscape, with many seeing a decrease in their ratings. Broker constraints and opportunities in special needs plans may also have some effect on payers in the MA space.
Payers may be in a rush to exit the Medicare Advantage market as they see its profitability declining, but this may not take place immediately. Medicare Advantage is still a massive part of the health insurance market that stands to continue profitability if payers can pivot their strategies, get creative with existing opportunities, and play with a straightforward hand.
The 2024-2030 plan lays out strategic goals and principles to help the health IT sector.
Last week the ONC released a strategic plan that outlines health IT priorities with a focus on health equity and AI use over the next five years. The plan intends to serve as a guide for federal health IT initiatives, as well as an impetus for activity in the private sector.
According to the ONC and HHS, the plan, which is a collaboration of the ONC with 25 other federal agencies, outlines federal health IT goals to improve health experiences and outcomes for individuals and populations as a whole.
The plan cites that its intended use aims to: prioritize resources, align and coordinate efforts, benchmark and assess progress, and signal priorities to the industry.
The plan outlines four main goals:
1. Health and wellness: Promote health and wellness for individuals, communities and populations so they feel empowered to manage their health.
2. Enhance the delivery and experience of care: Enhance the delivery of care for everyone from patients to providers to public health experts.
3. Accelerate research and innovation: Accelerate research and innovation through collaborative efforts across health IT developers and users.
4. Connect the health system with health data: Connect the health system with health data for all health IT users
Goals 1-3 are focused on plans to improve the experiences and outcomes for health IT users, while goal four focused on the policies and technologies needed to support those users.
The plan also outlines six principles including:
Person-centered, inclusive design to “strengthen individuals’ ability to securely access and use their own health information to take greater control over their own health, while ensuring that their data are accurate.”
Safety and quality to “promote the use of health data that are accurate and provide benefits to individuals and their communities.”
Privacy and security to “provide tools, guidance, and regulations to build trust and protect individuals’ health information from misuse.”
Data-led decision making to support health information sharing throughout the healthcare industry in order for groups, organizations and individuals make informed decisions and create better health outcomes.
Increase health equity across all populations to “advance the use of data to represent social needs and the conditions in which people live, learn, work, and play.”
Encourage innovation and competition to support “new solutions and business models for better care and improved outcomes.”
"The draft plan acknowledges the swift evolution of AI and increased use in health care, emphasizing the urgent need for the federal government to navigate this transformative landscape both responsibly and effectively in health and health care," ONC officials wrote in a blog post.
The affordability of health coverage is often a barrier for many.
The number of uninsured individuals in the US has slowly dropped over the last few years. Initiatives like the Affordable Care Act and enhanced subsidies in the Marketplace have helped millions obtain affordable coverage.
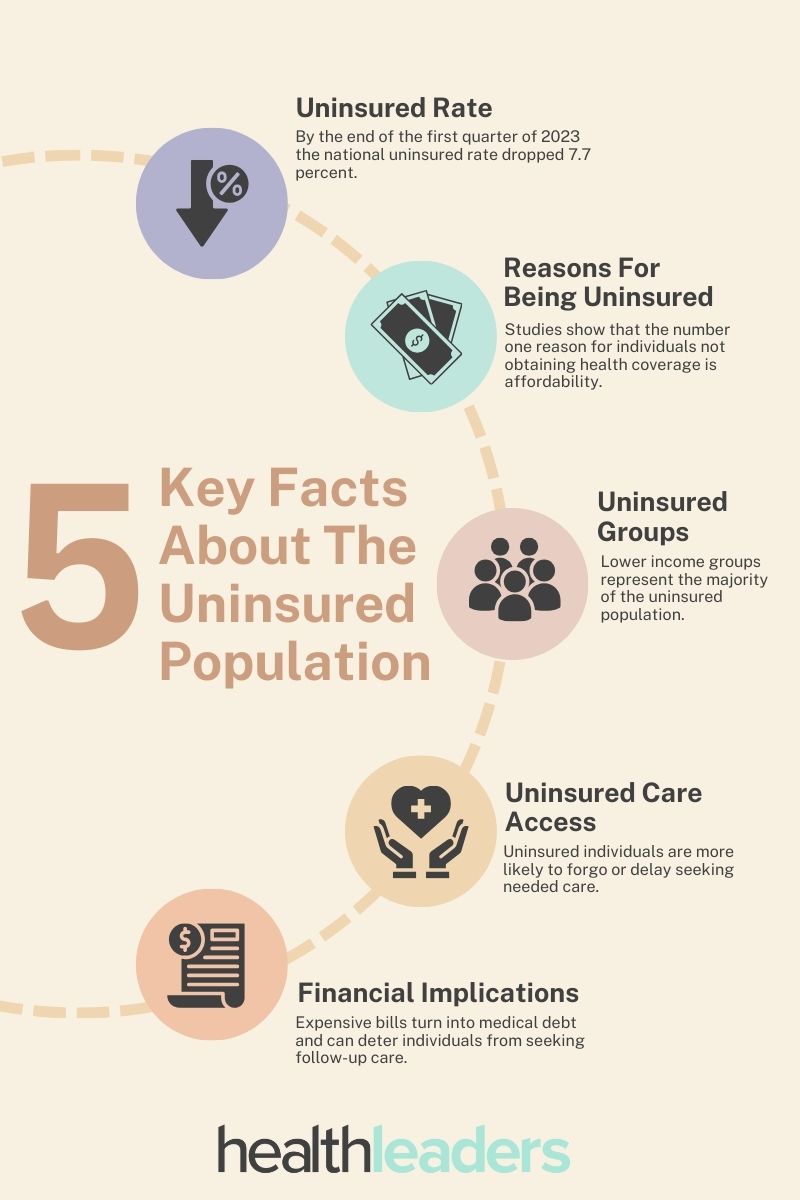
By the end of the first quarter of 2023 the national uninsured rate dropped 7.7 percent. Between 2020 and 2023 the total number of uninsured Americans declined from 31.6 million to 25.3 million.
The group with the highest enrollment rate were individuals whose income was either below 100 percent or between 200 and 400 percent of the federal poverty level. Racial and ethnic disparities in health coverage also persist, despite enrollment gains over time.
According to KFF, the cost of insurance is the number one reason for individuals not purchasing coverage is affordability. In 2022, 64 percent of nonelderly uninsured adults cited the high cost of coverage as their main reason for not purchasing insurance.
Many also cannot access coverage through their jobs, in states that did not expand Medicaid, many lower-income adults still remain ineligible for financial assistance for coverage. Up until recently, undocumented immigrants were eligible for federally funded health insurance, but some states like California, Oregon and Washington have taken aim at this issue and have offered extended coverage to immigrants.
The Biden administration has made healthcare a major focus of its term, and that has certainly played a role in increased enrollment. The significant enrollment gains in 2021-2023 can be associated with the administration’s policies to support health insurance expansion.
Individuals who do not have health coverage often forgo or delay seeking needed care and this only exacerbates the healthcare needs of the nation, leading to more hospitalizations and care team burnout. Numerous studies repeatedly show that uninsured individuals are less likely than the insured to seek or receive preventative care and other services for major health concerns and chronic diseases like diabetes and heart conditions.
Not being able to secure health coverage can have massive financial implications. When individuals without insurance do seek care, they're often faced with expensive bills that they cannot afford. Since most of the insured population is a lower-income group, seeking care can quickly turn into medical debt affecting other financial aspects of the individual's life and possibly deter them from seeking follow-up care.
Scams are on the rise and health insurance is no exception.
Picture this: you have a medical emergency, you head to a hospital, only to discover that your health insurance that you pay hundreds for each month doesn’t even exist.
The FTC is now sending out nearly $100 million in refunds to consumers that purchased fake health plans from Benefytt Technologies. The company and its third-party partners marketed and operated deceptive plans that targeted consumers searching for a comprehensive plan under the Affordable Care Act (ACA).
A 2022 FTC complaint details how Benefytt sales agents made telemarketing calls pitching their sham health plans that were not ACA-qualified. When consumers navigated the company’s websites, they were often led to a sales agent who would pitch them Benefytt’s unqualified, fake plans. Consumers were led to believe they were purchasing comprehensive plans for hundreds of dollars each month that in reality, left them with no protection in a medical emergency.
The Tampa-based company has been ordered to pay $100 million in refunds to consumers which included illegally charged junk fees for unwanted add-on products without their permission. In the settlement, Benefytt was also prohibited from lying about its products and charging these immense junk fees.
According to the FTC’s complaint, Benefytt’s deceptive sales process violated the FTC Act, the Telemarketing Sales Rule and the Restore Online Shoppers Confidence Act. All of these harmed consumers in numerous ways, such as: lying about the nature of the plans, bundling and charging junk fees for unwanted products without consent, and making it hard to cancel.
In separate court orders, Benefytt’s former CEO Gavin Southwell and former vice president of sales Amy Brady were permanently banned from selling or marketing any healthcare-related product. The former VP was also banned from telemarketing. Southwell acted as Benefytt’s president and CEO from 2016 to 2021 and Brady served as vice president of sales for more than a decade, before also leaving in 2021.
The complaint also alleges that Benefytt, Southwell, and Brady all were aware of their agent’s misconduct, but rather than stopping it, continued to profit from it and took steps to further conceal the deception. One example the complaint offered details how Benefytt assisted and facilitated the fraudulent offerings of one of their largest distributors, Simple Health Plans. Benefytt allegedly knew of the prevalent compliance issues with Simple Health’s sales practices, and failed to terminate the distributor until FTC sued Simple Health in October 2018.
Benefytt and two of its subsidiaries have agreed to a proposed court order that will require them to: pay $100 million for consumer redress, inform current customers and allow them to cancel, sell all products without misleading consumers, and closely monitor other companies who sell their products.
From an FTC press release: “Benefytt pocketed millions selling sham insurance to seniors and other consumers looking for health coverage,” said Samuel Levine, director of the FTC’s Bureau of Consumer Protection. “The company is being ordered to pay $100 million, and we’re holding its executives accountable for this fraud.”
Scams such as these are obviously dangerous and take advantage of consumers looking for comprehensive coverage. Payers should be aware of these events and do their best to educate their consumers of the dangers of online health insurance scams, as well as how to spot and avoid them.
The FTC offers a resource on their website to help consumers spot and avoid health insurance scams.
These two new smartphone apps may have a big impact on pediatric care.
New tech, including AI, has sailed its way from the conception phase, to implementation. So far this year two new smartphone apps are paving the way for small scale solutions that can have a big impact.
The first comes from the University of Pittsburgh where clinicians have developed an AI algorithm that can identify acute otitis media (AOM), one of the most common childhood infections.
Roughly 70% of children develop an ear infection before their first birthday. These infections are difficult to spot and distinguish from other types of infections that do not require antibiotics. But with this new smartphone AI tool, clinicians can more easily analyze a patient’s eardrum through an otoscope connected to a camera. The tool proved to have a 93% success rate at identifying AOM, versus expert physicians success rate at around 30% - 48%.
With implementation of this new tool, clinicians will no longer have to struggle to look in the ear of a wiggly infant to determine if they have an ear infection.
The second is an app developed by Intermountain Health that would help detect jaundice in newborns. Approximately three out of every five babies in the US develop jaundice within days after birth, which could lead to serious health concerns if not treated.
Intermountain Health partnered with a Norwegian digital health company called Picterus AS to create the app that uses a smartphone camera and a laminated card to measure bilirubin levels in newborns, allowing for a diagnosis without returning to the hospital for a blood test.
This new tech would allow parents to test their babies at home and alert care teams if jaundice is detected.
These two new smartphone apps may have a big impact on pediatric care.
New tech, including AI, has sailed its way from the conception phase, to implementation. So far this year two new smartphone apps are paving the way for small scale solutions that can have a big impact.
The first comes from the University of Pittsburgh where clinicians have developed an AI algorithm that can identify acute otitis media (AOM), one of the most common childhood infections.
Roughly 70% of children develop an ear infection before their first birthday. These infections are difficult to spot and distinguish from other types of infections that do not require antibiotics. But with this new smartphone AI tool, clinicians can more easily analyze a patient’s eardrum through an otoscope connected to a camera. The tool proved to have a 93% success rate at identifying AOM, versus expert physicians success rate at around 30% - 48%.
With implementation of this new tool, clinicians will no longer have to struggle to look in the ear of a wiggly infant to determine if they have an ear infection.
The second is an app developed by Intermountain Health that would help detect jaundice in newborns. Approximately three out of every five babies in the US develop jaundice within days after birth, which could lead to serious health concerns if not treated.
Intermountain Health partnered with a Norwegian digital health company called Picterus AS to create the app that uses a smartphone camera and a laminated card to measure bilirubin levels in newborns, allowing for a diagnosis without returning to the hospital for a blood test.
This new tech would allow parents to test their babies at home and alert care teams if jaundice is detected.
Britt Berrett dives into solutions for reducing expenses for health systems as payers and providers move towards contract negotiations.
Payers and providers must come to terms at the negotiating table, and reducing expenses is an item that directly benefits both parties.
HealthLeaders spoke with Britt Berett, Managing Director and Teaching Professor at Brigham Young University, to hear his insights on what solutions payers and providers must work towards, and the options they will need to explore in order to reduce expenses this year.
Some states are hesitant to cover the popular drugs.
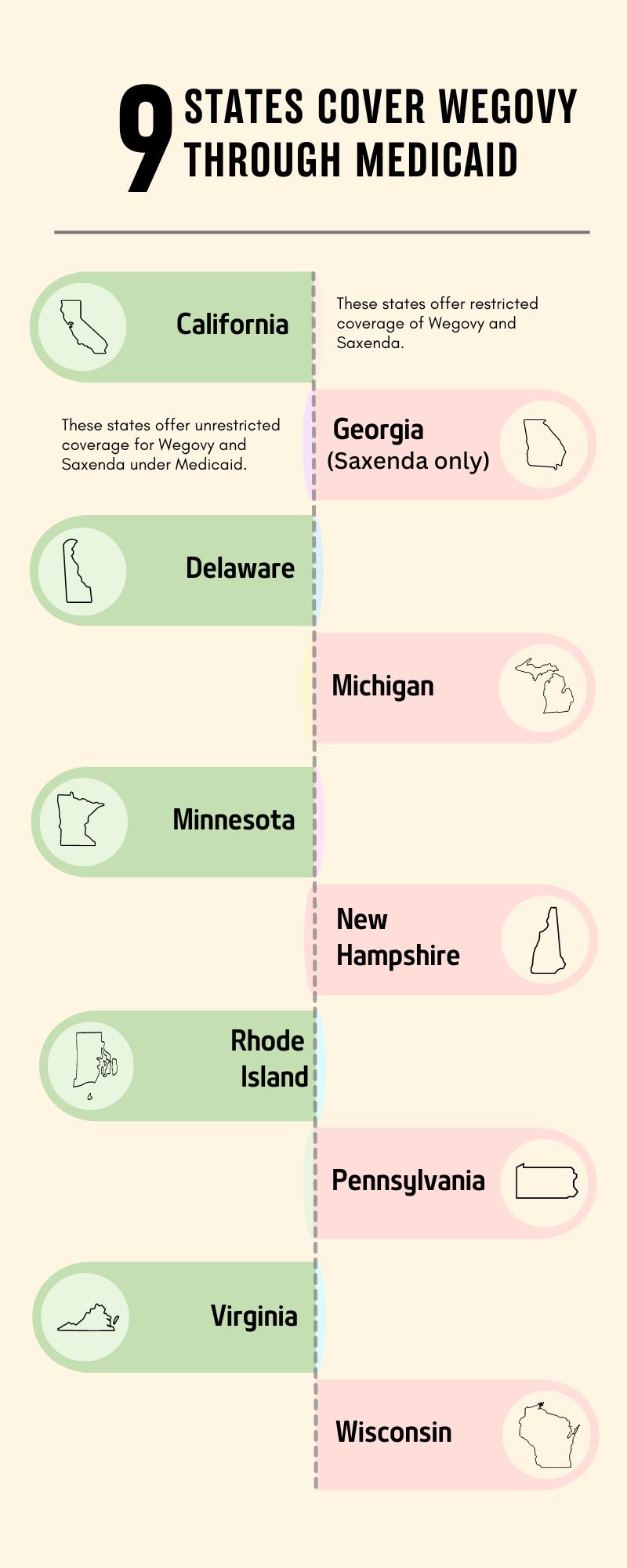
Weight loss drugs have soared in popularity; while some states have been hesitant to cover them, others have not. A recent JAMA study found that five states offer unrestricted coverage of GLP-1 drugs Wegovy and Saxenda that were approved for weight loss.
The data from this study comes from formularies for 47 state Medicaid programs from the first quarter of 2023.
The study found that a total of ten states cover Saxenda or Wegovy for weight loss, while five of those states offered restricted access through barriers like prior authorization, non-prefered status, or step therapy.
Some GLP-1 drugs approved for coverage to treat diabetes such as Ozempic, Victoza or Trulicity, are covered in 39 states.
Some states are hesitant to cover these popular drugs because of the hefty $15,000 price tag that accompanies them.
As 2023 these five states offer unrestricted coverage to Wegovy and Saxenda under Medicaid:
California
Delaware
Minnesota
Rhode Island
Virginia
These five states offer restricted coverage of Wegovy and Saxenda:
A new report shows strong potential for the Medicare Advantage market.
There are a number of items shaking up the Medicare Advantage space lately, from steeper star ratings to broker constraints. However, a new report has an optimistic outlook for MA, even as growth begins to slow down.
Findings in a recent report by Chartis show that Medicare Advantage growth seems to be slowing, despite enrollment gains. In 2023 MA grew by about 5%, or 1.7 million new members, slower than the year before which was at around 9%, or 2.7 million members. The rise comes from a growing senior population, yet has been overshadowed by factors like regulatory pressures, decreased star ratings, and soaring medical costs.
A majority (86%) of the market’s growth in the past year has come from for-profit insurers like Humana, Aetna and UnitedHealth. Collectively, these three giants captured 1.4 million new beneficiaries. This enrollment growth follows a big MA milestone of over 50% of Medicare-eligible persons enrolling in an MA plan.
According to the Chartis survey that looked at 19 insurers, even with a decrease in growth, almost 80% of health plan executives were optimistic about the next five years, and they are expecting neutral or positive outcomes. Roughly 84% also anticipate membership growth that is equal to or greater than this year, showing payer confidence in the stability and overall growth potential of the Medicare Advantage market.
Ratings
Medicare Advantage has wrestled with many different opponents, such as new methods of calculating star ratings. During the pandemic when relief provisions were high, MA ratings shot up. As regulators noticed this and pulled back on them, they started new methods of calculating ratings, which then fell for many insurers. Elevance even went through a lawsuit with HHS over their low ratings and managed to come out with new ratings and a hefty payout. Quality of plans remains a concern as plans struggle to maintain high quality ratings, with roughly one-quarter of beneficiaries enrolled in a plan with less than four stars, according to the report.
Special Needs Plans and Social Vulnerability
Special needs plans are also gaining more traction in the Medicare space. The Chartis report looked at SNPs which have recently surged, with an addition of over 1M new members. Almost 7 out of every 10 MA enrollees opted for SNPs.
The report also dug into another not-so-obvious factor, the relationship between MA enrollment and social vulnerability. It found the counties with higher vulnerability scores showed greater penetration rates, about 53%, when compared to counties with lower scores, about 45%. These statistics show how market dynamics are playing into the greater picture of MA.
Nick Herro is the Chartis Director in Strategic Transformation and co-author of the report. He says that although the MA market has matured a great deal over the last several years, demand continues mainly due to changing demographics and consumer preference over traditional Medicare.
"We are confident demand for Medicare Advantage will hold steady,” Herro said in a press release. “While plan executives acknowledge the headwinds facing the industry, the majority express optimism about the next five years."
Taking all of these factors into consideration, the Medicare Advantage market could gain even more traction and attention from payers as outlook reports seem promising. However, maintaining high quality ratings and keeping up with the demand and shifting market dynamics could outweigh the promise of stability and growth potential of the market.
U.S. officials are putting the pressure on payers to take more targeted action.
This week payers met with federal officials to discuss how they can advance timely payments to providers who are still struggling after the massive cyberattack on Change Healthcare.
Payers were asked to prepare details on how they plan to financially support providers, how they are working to meet the challenges, and recovery efforts that still need to be made.
Payers are concerned about how their money will be recuperated in the future, according to a report from Bloomberg.
HHS has urged payers since the beginning of the attack to help providers by removing or relaxing prior authorizations, but the pushback has been strong. AHIP President and CEO Mike Tuffin issued a statement on March 12 about insurers responding to the attack.
Since the impact varies across their system, United urged individual plans and providers to sort out payments in a timely manner, as they’re in the best position to do so.
“Further, broad exemptions in prior authorization at a time of advanced payments could expose patients and employers to fraud, waste and unnecessary costs,” said Tuffin.
In a press release, the organization announced it will be launching software for preparation of medical claims and announced that it has advanced $2B to providers who are still struggling after the attack. The software will be made available to thousands of customers over the next several days and it expects to have third-party attestations available before these services become operational. After this initial phase, other restoration services will continue until all its customers have been connected.
UnitedHealth has also been reported as offering substantial loans to some providers after the cyberattack. Stat News reported that this change comes as hospitals, doctors and lobbying groups have complained for weeks about United’s low offers, some less than 1% of their regular weekly billing. Now, some providers have seen their advances increase up to seven figures, but we’re not sure why or what prompted these specific loans.
But What About The Other Payers?
UnitedHealth seems to be making headway on helping their providers, but what about other payers? During the March 18 meeting, several payers said they would commit to advancing payments to providers, but these payers were not named.
According to Reuters an unidentified U.S. official said, "Claims are starting to flow and we have seen significant improvement between last week and this week, but we have a last mile to go.”
In a press release HHS said that it surveyed payers in their previous meeting to obtain data and information that showed the actions they are taking to resolve issues from the cyberattack. HHS reviewed the responses over the weekend of March 15. Payers then offered HHS updates on their resolution efforts towards providers and outlined specific actions they plan to take.
“HHS and White House leadership pressed insurers to be targeted and specific in carrying out solutions, including increasing advanced payments where needed to the providers and communities still most in need,” HHS said in the press release.
As health systems slowly begin to get back on track with payments and regular operations, it’s clear that payers have been slow to act in this crisis and give aid to their providers and patients. As payers look for a balance between advancing payments without advancing fraud in this difficult situation, some providers are still struggling to keep their systems operational without the cash flow.




e40c.jpg)






8b17.jpg)